- Citas Centro Médico de Caracas: Lunes, Miercoles y Viernes. Pulse el botón Agende una Cita
- Sistema de citas en linea exclusivo para Centro Medico de Caracas en San Bernardino
- Citas CMDLT: Jueves. llamar al 0212-9496243 y 9496245
- Las Emergencias son atendidas en CMDLT previa coordinacion personal al 04142708338
- Proveedor Seguros Mercantil y Sudeban

Systemic Lupus Erythematosus (SLE) is an autoimmune disease that primarily affects women of reproductive age (Female / Male 9: 1). It produces variable and episodic chronic inflammatory phenomena (flares), direct cell damage mediated by antibodies or cells (toxicity: hemolysis, thrombocytopenia) and / or mediated by circulating immune complexes. The disease affects many organs and systems (skin, joints, kidneys, brain, formed elements of the blood and serous membranes) through a chronic inflammatory mechanism generated by the immune response against the tissues themselves. One of the most striking elements is the large profusion of antibodies against the patient’s DNA.
Exacerbations (Flares) appear to correspond to acute immune responses due to acute aggression such as ultraviolet (sun) injury, common viral infections, cyclic menstrual or breast cycle changes
Although LES does not seem to directly affect fertility, some treatments of the disease may affect the ovarian reserve (cyclophosphamide).
Pregnancy carries greater risks for the lupus woman. Maternal-fetal prognosis is better in women with silent disease at least six months before pregnancy. The typical exacerbations of the disease do not seem to be more frequent during pregnancy but if there is no suspicion they can be eclipsed by the changes inherent to pregnancy.
Emergency:
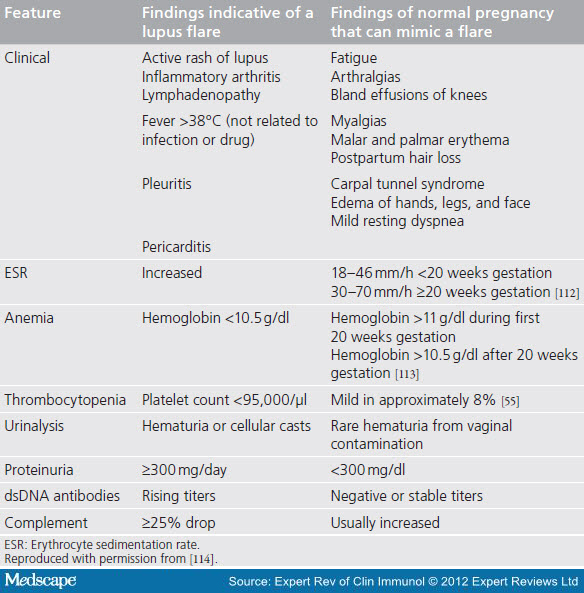
Lupus flare: differences with gestational changes
{kind=link}
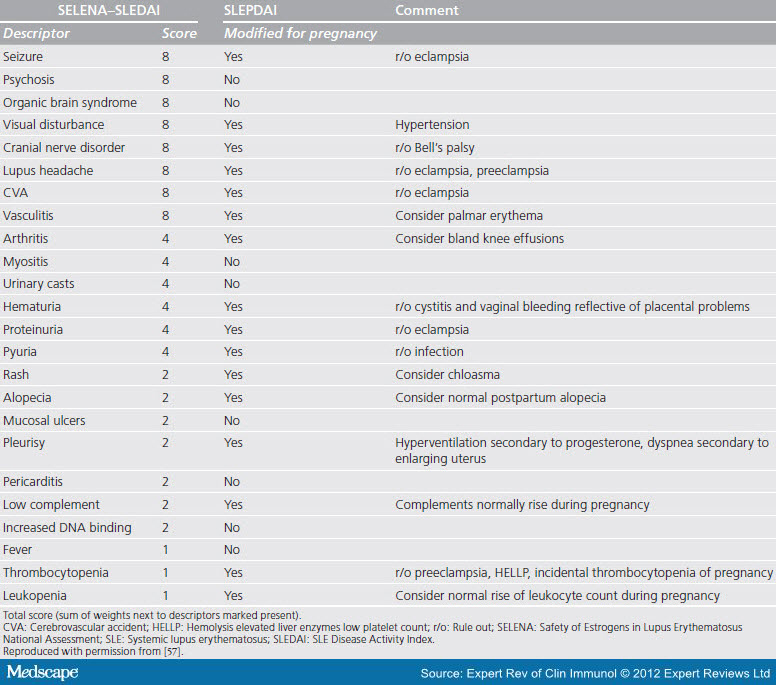
Selena-Sledai : score, criteria
{kind=link}
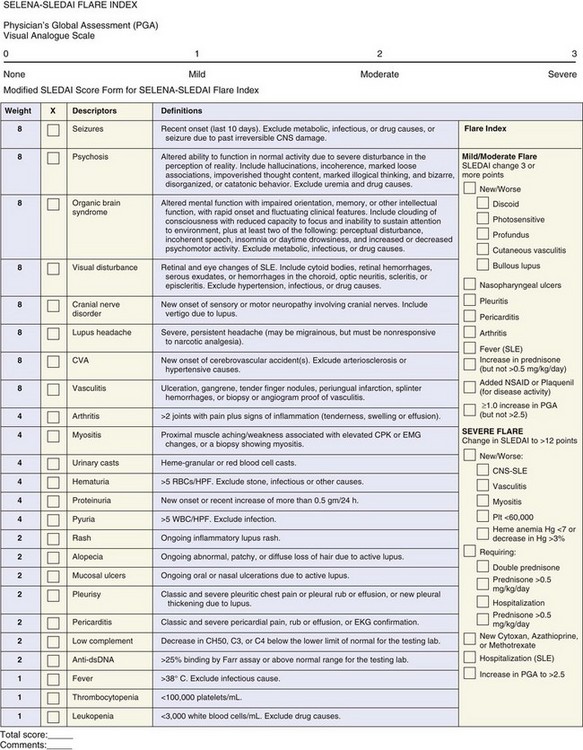
Slepdai: checklist
{kind=link}
CLINICAL MANAGEMENT
I PRECONCEPTIONAL
The best maternofetal prognosis is observed when the woman becomes pregnant with at least 6 months of lupus inactivity, the peror, when she becomes pregnant during the activity (clinical or biochemical evidence of flares or exacerbations). Despite this, most patients will achieve a live birth:
385 lupus patients with inactive, mild or moderate disease: excellent evolution with 81% of pregnancies without obstetric complications , 88% live births. What we must face: hypertension, preeclampsia, fetal growth retardation, prematurity
267 lupus patients with severe active disease: the adverse results were much more frequent with 45% of abortions and fetal loss and frequent obstetric complications; however, 77% of live births
1.- Clinical evaluation –
Discard flares
Transition to safe medications in pregnancy
Determine damage to organs associated with SLE: lupus nephritis is the element that most often dictates the prognosis of pregnancy, in its presence should contraindicate pregnancy. Once controlled, the patient must wait at least 6 months to consider the pregnancy. Kidney failure can be exacerbated and lead to a myriad of maternal-fetal complications
Determine hypercoagulability, antiphospholipid syndrome,
Determine the presence of other concurrent diseases
Results of past pregnancies: recurrent abortion, fetal death, IUGR / PEG, HIE, prematurity
The pregnancy must be contraindicated in: renal failure
2.- Laboratory – to include in the preconceptional laboratory
1.- Antibodies:
Antiphospholipid antibodies (aPLs): Lupus anticoagulant (AL), Anticardiolipin (aCL), Anti B2 Microglobulin. Related to IUGR, recurrent fetal loss, preeclampsia)
Neonatal Lupus Antibodies: Anti-Ro / SSA and anti-La / SSB antibodies. They lead to Neonatal Lupus: complete AV block
Antibodies double helix DNA: Anti-dsDNA:
2.- Renal Function: Urea, Creatinine, Uric Acid, Urinary Sediment, P / Cr Index
3.- Complete hematology
4.- Liver profile
5.- Complement (CH50, or C3 and C4)
3.- Medications – Select the safest for the fetus
Recommended:
Hydroxichloroquine – Better pregnancy prognosis, fewer flares, lower dose of prednisone, better evolution during the puerperium, lower fetal heart block in anti-Ro / La positive mothers
Aspirin – From week 12 regardless of the aPL status, 81-150 mg per day
Use with caution:
Non-steroidal anti-inflammatories – Can be used before 32 weeks of pregnancy with caution. After, only with permission of the obstetrician
Glucocorticoids – Cautious use, ideally a daily dose of less than 10 mg
Azatioprine – Relative safety, dose less than 2 mg / kg / day.
Ciclosporine – When the benefit outweighs the risk
Tacrolimus – When the benefit outweighs the risk
Antihypertensives – Methyldopa, labetalol, nifedipine, and hydralazine are the safest
Biological – Limited experience
Contraindicated
Cyclophosphamide, Mycophenolate mofetil, Methotrexate, Leflunomide
II SPECIFIC CONSIDERATIONS DURING PREGNANCY
1.- Exacerbation of SLE – It is possible that pregnancy and puerperium raise the frequency of exacerbations to 25-60%; the usual annual, outside of pregnancy is 30%. The risk factors are:
Primigesta, nephritis, HCQ suspension and initiate pregnancy with disease activity or less than 6 m, since the last crisis
2.- Impact of lupus on pregnancy – 2-4 times greater risk of prematurity, emergency cesarean section, IUGR, preeclampsia (PE), eclampsia , thrombosis, infection, thrombocytopenia and transfusions (postpartum hemorrhage) . Maternal mortality is also increased
3.- Prematurity – It is the most frequent complication, 15 to 50% (compared to 5-10%), mostly iatrogenic, due to the interruption of pregnancy due to disease activity, placental abruption (DPP), fetal distress and preeclampsia
4. Preeclampsia – It occurs in 16 to 30% of women with SLE, compared to 4.6% of women without the condition. HELLP syndrome can overlap or confuse a flare
5.- Fetal Complications and Death – Abortion, fetal death (5%), prematurity, IUGR (10 – 30%), low weight for gestational age (PEG) and Neonatal Lupus. Fetal death after week 10 is particularly known in SLE, antiphospholipid syndrome and lupus nephritis
8.- Neonatal Lupus – Due to the anti-Ro / SSA and / or anti-LA / SSB the manifestations are cutaneous, cardiac (2% of the neonates, the most feared.In the following pregnancy it can be 14-16%) , hematological and hepatic.
III SPECIAL CONSIDERATIONS
1.- Lupus Nephritis – Defer pregnancy until at least 6 months of inactivity to reduce the general risks during pregnancy (43 vs 88%), Flares (25 vs 54%), Preeclampsia (35 vs 57%), prematurity ( 30 vs 52%), abortions (25 vs 35%). Fortunately, almost all responded to high doses of prednisone and there were no pregnancy losses
2.- Presence of Anti Phospholipid antibodies (aPLs) – present in 25-50% of patients with SLE very few will develop thrombotic complications related to these antibodies
Its presence should be considered in: habitual abortators (> 3 abortions), fetal deaths after week 10, premature partp before week 34, preeclampsia, placental insufficiency, IUGR or unexplained arterial or venous thrombosis.
3.- Presence of anti-Ro / SSA and anti-La / SSB antibodies – Fetal risk of LN and AV blockade between weeks 18 and 24. There is no therapy for this condition but HCQ seems to exert a protective effect. Even when they are secreted in breast milk, they do not seem to cause problems in the infant
IV HANDLING DURING PREGNANCY
1.- Monitoring of Lupic activity – Surveillance of lupus activity every 3 months or in each trimester
initial evaluation
Physical exam
Kidney (creatinine, urinalysis with sediment, urinary protein / creatinine index)
Complete hematology
Liver profile
Anti-Ro / SSA and anti-La / SSB
Lupus anticoagulant (LA) and anticardiolipin
Anti-double-stranded DNA (dsDNA)
Complement (CH50 or C3 and C4)
Uric acid
Note: the supplement can increase 30-50% during pregnancy so that during an exacerbation its decrease can be within normal levels.
Monthly controls
Physical exam
Kidney (creatinine, urinalysis with sediment, urinary protein / creatinine index)
Complete hematology
Quarterly laboratory
Anti-double-stranded DNA (dsDNA)
Complement (CH50 or C3 and C4)
Note: laboratory control can be quarterly; in case of activity, monthly controls can be carried out according to the rheumatologist’s criteria
Postpartum assessment
Evaluation is recommended one month after birth:
Kidney (creatinine, urinalysis with sediment, urinary protein / creatinine index)
Complete hematology
Liver profile
Anti-double-stranded DNA (dsDNA)
Complement (CH50 or C3 and C4)
Uric acid
Breastfeeding may be contraindicated by certain medications
2.- Maternal-fetal monitoring – The control requires a specialist in advanced structural and functional surveillance of the fetus, usually following the same pattern of control that a specialist in this category would maintain on all his patients.
In our particular case we perform monthly echographic evaluations that include fetal Doppler from the first evaluation to determine elements of embryonic prognosis (4 to 10 weeks)
Genetic Ultrasound of the First Trimester (11-13.6 Scan)
Monthly sonography, includes spectral color Doppler and other functional evaluations
Risk assessment of Trecer Trimester between weeks 24-28: Doppler profile, fetal echocardiography, neurosonography, cervicometry, detection of preeclampsia. In patients with anti-Ro / SSA and / or anti-La / SSB we practice M mode to assess heart rate.
In case of IUGR with alterations in the fetal circulatory profile, the patient is evaluated weekly and even more frequently in the case of imminent interruption. All available sonographic resources are used
3. Preeclampsia – because its risk is greater ( 16 to 30% ) preventive measures (Aspirin 81 mg / day from the beginning of pregnancy, reduction of 24% of cases of PE) and diagnostic should start early. If PE appears towards the end of pregnancy, management can be conservative; if it occurs far from the term, control is aggressive to avoid catastrophic complications and try to prolong pregnancy as long as possible for fetal reasons. The mother is a priority
4.- Preeclampsia versus lupus nephritis – Differentiating the changes of normal pregnancy with some data of lupus activity can be difficult, differentiating them from PE, quite a challenge
| Clinical and Laboratory Features | Pre-eclampsia | Lupus nephritis |
|---|---|---|
| Hypertension | After 20 weeks of gestation | Any time during the pregnancy |
| Platelets | Low – normal | Low – normal |
| Complements | Normal – low | Low |
| Anti dsDNA | Absent or unchanged | Rising titers |
| Creatinine | Normal – raised | Normal to raised |
| Serum Uric Acid | Elevated (> 5.5mg / dl) | Normal |
| 24 hour Urine Calcium | <195mg / dl | > 195mg / dl |
| Urinary Sediment | Inactive | Active |
| Other Organs Involved | Occasionally CNS or HELLP | Evidence of active non-renal SLE |
| Response to steroids | Do not | And it is |
One of the most sensitive data to differentiate both conditions is the detection of cell cylinders in the sediment.
5.-Symptoms – Differentiation of the lupus activity of pregnancy changes
| Characteristic | Pregnancy-related changes | SLE flare |
|---|---|---|
| Mucocutaneous | Facial flush Palmar erythema Postpartum hair loss |
Photosensitive rash Oral or nasal ulcers |
| Musculoskeletal | Arthralgias Myalgias |
Inflammatory arthritis |
| Hematologic | Mild anemia, Mild thrombocytopenia | Leukopenia, lymphopenia Immune hemolytic anemia Thrombocytopenia |
| Renal | Physiologic proteinuria <300mg / day | Active urinary sediment Proteinuria> 300mg / day |
| Immunologic | Higher complement levels | Falling complement levels Rising anti DNA levels |
| Others | Fatigue Mild edema Mild resting dyspnea |
Fever Lymphadenopathy Pleuritis |
6.- Treatment of lupus activity – The selected treatment must be safe for the fetus but often the risk should be weighed when it is necessary to use potentially harmful drugs for the fetus, it is better to deal with a potential risk to a catastrophic maternal complication that I could quickly end the life of both.
V LACTATION
Breastfeeding should only be stopped by the use of certain medications. Most of the patients will be able to breastfeed without problems since most of them will have safe treatments for lactation: Hydroxychloroquine (HCQ), prednisone, cyclosporine, azathioprine, tacrolimus and methotrexate in low and intermittent doses are compatible with breastfeeding.
Cyclophosphamide contraindicated