- Citas Centro Médico de Caracas: Lunes, Miercoles y Viernes. Pulse el botón Agende una Cita
- Sistema de citas en linea exclusivo para Centro Medico de Caracas en San Bernardino
- Citas CMDLT: Jueves. llamar al 0212-9496243 y 9496245
- Las Emergencias son atendidas en CMDLT previa coordinacion personal al 04142708338
- Proveedor Seguros Mercantil y Sudeban
Gestational Diabetes (GD) refers to the appearance of high blood sugar levels in a previously normal pregnant patient due to an exacerbation of insulin resistance due to the effect of placental hormones, an increase in body fat and the inability of the maternal pancreas to deal with these changes. They are healthy patients who begin to manifest hyperglycemia during pregnancy without having a personal history of diabetes. Usually the patient has no idea of ??what is happening (totally asymptomatic) and the diagnosis is made during the screening of diabetes in the weeks 24-28 of the current pregnancy.
Pregestational Diabetes (PGD) refers to Diabetes Mellitus that predates pregnancy, the term helps to establish that the pregnant patient was known to be a carrier of some form of Diabetes Mellitus and that it has the inherent risks of long-standing hyperglycemia (including severe fetal malformation) , in most cases they are young women with Diabetes Mellitus type 1 and to a lesser extent they are women a bit more mature, overweight or obese carrying Diabetes Mellitus type 2.
Maternofetal complications depend on the type of diabetes present, in general GD does not induce fetal problems beyond those related to obstetric trauma due to the birth of bulky fetuses (macrosomic), caesarean section and postnatal risks associated with obesity and future diabetes
Frequency and generalities
It is common and complicates approximately 5% of all pregnancies. It is a type of diabetes exclusive of pregnancy that is defined as carbohydrate intolerance (elevated plasma glucose during fasting and / or after each meal) with variable severity that begins or is initially recognized during pregnancy. Because of its frequency and the maternal-fetal problems it produces, it is indicated to perform specific studies to rule out or detect its presence routinely, as part of prenatal control during pregnancy, in the period between 24 and 28 weeks. Fortunately, it is easy to use and its complications are scarce or nonexistent if the diagnosis is made at the time. It is important to mention that those patients who suffer from gestational diabetes have a high risk of suffering from Diabetes Mellitus (usually type 2) in the near future if they do not change some habits in their daily routine of life
Effects of Gestational Diabetes on the fetus
Gestational diabetes is manifested by high levels of maternal glucose that will pass to the baby and make it grow excessively fast, although this seems very nice the fact is that these babies (called macrosomic because of their large size and weight greater than 4 – 4.5 kg), not only are they at risk of complications from trauma during birth (shoulder dystocia, obstetric trauma, clavicle fracture, perinatal asphyxia) and a high rate of caesarean sections, but immediately after birth can present serious metabolic problems (reactive hypoglycemia, hypocalcemia , respiratory distress) that can endanger your life; In addition, it is now known that macrosomic babies have a greater future risk of manifesting diabetes and other diseases: obesity, hypertension, cardiovascular diseases, certain types of cancers, etc.
Maternal hyperglycemia leads to fetal hyperglycemia which in turn will lead to fetal hyperinsulinemia and finally to excessive accumulation of fetal body fat, iron deficiency in key organs for fetal development and enlargement of the liver, spleen and heart. All this accelerated metabolic environment translates into excessive oxygen consumption and fetal hypoxia, iron deficiency and neurodevelopmental disorders of the fetus (memory and learning), the most critical period occurs during the third trimester of pregnancy so the glycemic control must be more strict at the end of pregnancy.
Effects of Gestational Diabetes on the mother
- Prolonged delivery and greater possibility of an emergency cesarean section due to a large fetus.
- Obstetric genital trauma due to the vaginal birth of a bulky baby: tears, hemorrhages, infection, prolapse, incontinence, etc.
- Type 2 diabetes in the near future: 50% risk at 5 years of the baby’s birth.
What is the treatment of Gestational Diabetes?
If you are diagnosed with Gestational Diabetes you may be able to control your blood glucose levels through a healthy and balanced diet accompanied by regular exercises .
If these measures are insufficient, we add oral hypoglycemics with excellent and easy glycemic control in most of the patients.
In some cases it is necessary to use insulin during the rest of the pregnancy in order to control blood sugar levels. The good news is that once the pregnancy is over you will no longer need insulin as long as you maintain a healthy habit of life away from obesity and sedentary lifestyle. Most women with gestational diabetes will have healthy babies if the diagnosis is made early, problems occur when it is not diagnosed or treated properly.
Currently and by virtue of the prevention of complications of diabetes the tendency is to be more aggressive in glycemic control.
Patients with any form of diabetes in pregnancy should follow the following guidelines and take the following steps:
- Glycemic control:
- Fasting : less than 95 mg/dL
- 1 hour after eating : less than 140 mg/dL
- 2 hours after eating : less than 115 mg/dL
- Changes in diet, healthier food and low glycemic index; consult a nutritionist.
- Exercise daily, can begin with 30 minutes after each meal to help glucose metabolism during absorption.
- If diet and exercise do not allow you to maintain glycemia according to the objectives described above you should start using metformin.
- The option of using insulin should be offered if, despite following all the measures described, the glycemic control described can not be maintained.
- Insulin should be indicated immediately, with or without metformin, to those patients who at the time of diagnosis have fasting glycemia figures of 126 mg/dL or greater.
- Consider the use of glibenclamide in patients who do not tolerate or do not respond adequately to metformin or who refuse to use insulin.
- The measurement of glycosylated hemoglobin is not indicated as a monitoring element of the glycemic control of the pregnant woman with GD, it is indicated in the pregestational diabetic.
Prevention
Do not give in to the impulse of the “cravings for pregnancy”: remember, pregnancy does not give you the right to gain irresponsible weight . Place your weight gain within reasonable levels established for your body mass index.
Choose healthy foods and plan a balanced diet. Do not eat “junk”: fast foods are the product of a very specialized design to achieve great sales due to its high addictive level due to the high levels of insulin that trigger and reactive hunger in 2 hours.
Avoid sodas, processed juices and natural juices: water is always the best liquid to ingest and does not get fat.
It is important to eat at the same times each day. For example, you could have breakfast at 7 in the morning, lunch at noon and dinner at 8 at night. Take small snacks at 10:00 in the morning and 5 in the afternoon. Intake at regular intervals helps maintain stable levels of glycemia. Avoid foods with a high glycemic index.
Accustomed to exercise regularly: not only helps control your weight but also improves your cardiovascular condition and also increases your chances of having a satisfactory vaginal delivery (better muscle tone and pain tolerance); There is even research that suggests that exercise during pregnancy has a positive effect on the physical development of your children after birth.
Ask or remind your doctor to order the Gestational Diabetes screening test (it should be routine between weeks 24 and 28)
Baby’s birth
In patients with gestational diabetes, the interruption of pregnancy is recommended elective before week 41, either delivery or cesarean, according to obstetric indication
In PGD patients pregnancy should not exceed week 38.6
After birth
We suggest changes in lifestyle habits, diet, exercise and weight loss.
It is recommended to practice a fasting glycemia at 6-13 weeks (in the postpartum visit of 6 weeks it is convenient to ask for it) in those patients who suffered GD.
After week 13, a fasting glycemia or a glycosylated hemoglobin (HbA1c) can be requested.
It is not recommended to practice routine glucose loading in patients who suffered GD.
It is recommended to practice glycosylated hemoglobin (HbA1c) annually to patients who suffered GD but whose postnatal glycemia controls were normal.
Forecast and future
At the end of pregnancy, Gestational Diabetes disappears, if not all, in the vast majority of them but if you do not take care of yourself (healthy diet and exercises, far from overweight, obesity and sedentary lifestyle) you could manifest type 2 diabetes (and its complications) after a few years (50% at 5 years).
Do not miss this warning!
NICE guideline
New guidelines : NICE study February 2015. I am using new English guidelines for use in my patients. It is comprehensive and considers the patient before, during and after pregnancy. The problem I must consider is that it eliminates the condition “Carbohydrate Intolerance” and adjusts the value afterload to a lower limit, which could increase the number of cases diagnosed with DG. We will discuss which scheme we will use but we may use this for the patient’s convenience
Diagnosis : one step, one single screening and diagnostic test
Interpretation : DG is diagnosed with only one altered value
Fasting: greater than or equal to 101 mg / dL
2 hours : greater than or equal to 140 mg / dL
NICE Guideline, February 2015, National Institute Health and Care Excellence. United Kingdom https://www.nice.org.uk/
*
Glucose overload 50 grams (G50, Glucola 50)
This is the routine test that should be practiced to every pregnant woman between weeks 24 and 28. The screening should be done in the entire Hispanic population and is based on the ingestion of 50 grams of glucose and the measurement of blood glucose exactly 1 hour later. You can measure glycemia before fasting but it is not absolutely necessary. This is the old standard but I moved to the NICE protocol
Normal value: 130-140 mg / dL
Results / Risk
According to the values ??obtained by the Glucose 50 Overload test, the risk of suffering from Gestational Diabetes (GD) in pregnancy can be predicted. When the values ??approach 200, we make the diagnosis without asking for other tests
|
Value (mg / dL)
|
Risk DG
|
|
135-144
|
14.6%
|
|
145-154
|
17.4%
|
|
155-164
|
twenty%
|
|
165-174
|
28.6%
|
|
175-184
|
fifty%
|
|
> 200
|
100%
|
**
If the screening test yields a positive risk result, the following diagnostic test should be performed:
Glucose overload G75 or G100
To make the diagnosis of GD, a CTOG (oral glucose tolerance curve) is practiced 2 or 3 hours after having ingested 75 or 100 grams of pure glucose. The normal values ??are those described by the National Diabetes Data Group (NDDG) and those proposed by Carpenter and Coustan (C & C)
Referential values
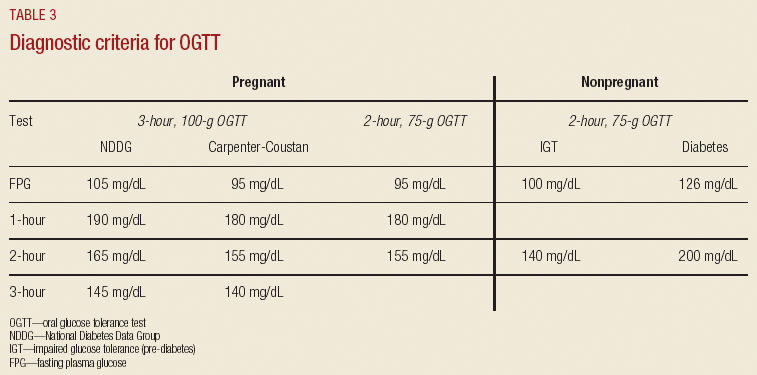
Interpretation:
Glucose intolerance: 1 abnormal value
Gestational Diabetes: 2 or more altered values

**
Bariatric Patients, weight loss surgeries
These tests may have errors in their interpretation and there is no consensus on their effectiveness in this population; however, it is the only available and can be useful by carefully interpreting your results
*
Diabetes in Pregnancy , 2018