- Citas Centro Médico de Caracas: Lunes, Miercoles y Viernes. Pulse el botón Agende una Cita
- Sistema de citas en linea exclusivo para Centro Medico de Caracas en San Bernardino
- Citas CMDLT: Jueves. llamar al 0212-9496243 y 9496245
- Las Emergencias son atendidas en CMDLT previa coordinacion personal al 04142708338
- Proveedor Seguros Mercantil y Sudeban
After 10 weeks of pregnancy, the embryo is now a fetus, organogenesis has ended and the baby acquires human form. Between weeks 11 and 13.6 we have the best and earliest possibility to detect/suspect multiple fetal problems of chromosomal, genetic and congenital origin thanks to the 11-14 Scan (Fetal medicine foundation). In general, detection approaches 95% with 2.5% false positives. When only maternal age is considered, amniocentesis is indicated in 15-20% of pregnant women with a detection of chromosomal syndromes in less than 50% of the cases studied. Using the tests described in this article, we decreased the frequency of amniocentesis to 3% with detection rates greater than 95%.
In many countries where the number of pregnant women under 35 years is high (90-95%), 75% of the cases of chromosomal syndromes will be found in their group, and only 25% in the 35+ y/o group. That is why every pregnant woman should be studied regardless of her age, forgetting the unsafe precept that stated “young women are not at risk of having babies with Down syndrome” and change it for “any and all pregnant women have a fetus with malformations (chromosomal and many others) until proven otherwise”.
Because the number of pregnant women older than 35 years is increasing (about 20% in developed countries), 50% of cases of chromosomal syndromes are present in this age group and the remaining 50% in women under 35 years of age.
Warning: These are Screening Tests that measure the risk of suffering a disease, therefore they do not diagnose any chromosomal problem. If the test suggests high risk, a Diagnostic Test (example, Genetic Amniocentesis) should be performed before making any decision. If the findings suggest a specific malformation, a presumptive or definitive diagnosis can be made.
A great study for your peace of mind
The Genetic Scan represents one of the most recent advances in the early suggestive diagnosis of fetal chromosomal abnormalities in modern Obstetrics. Officially known as the 11 to 14 Week Evaluation (“The 11-13 + 6 Week Scan” of the Fetal Medicine Foundation, UK) or First Trimester Genetic Sonography, behaves like a very well structured and standardized evaluation of the fetus from 11 to 13.6 weeks in order to detect small markers that may suggest the presence of Chromosomal Abnormalities, some Genetic Syndromes and evident Congenital Abnormalities. As a secondary gain, fetal sex can be established with 98% accuracy (after week 12). Watch a brief video of this period (Thanks to Aracelis).
The best time to perform the ultrasound is at week 11 but since the fetus looks better seen at 12 weeks, we prefer this gestational age. We have observed the same detection throughout the period (11 to 13).
This is a very limited time window of invaluable value that has proven to be one of the best moments to detect fetal problems, in fact, it is the period where there is the highest known capacity for detection of Down Syndrome (Trisomy 21, T21) with rates that exceed 80%. This means that if the baby is a carrier of the Syndrome we could detect it with at least 80% probability. And better yet, if all markers are normal we could rule out chromosomal problems with 90-100% specificity.
How does the Genetic Scan work?
Babies with chromosomal problems show certain anatomical and functional elements that can be detected during this period using high resolution sonography. In our Service we start the study via the Transvaginal route (USTV) to take advantage of the higher resolution of intracavitary transducers and then we complement it using the abdominal route (USTA). During the study we discard the presence of Fundamental Markers and General Markers (own classification) and all possible anatomical and functional data
I Fundamental Markers: are four (4) markers that have the highest detection capacity. If an alteration is determined in one or more of them, an invasive diagnostic test will be suggested or a follow-up protocol will be followed to rule out false positives. Each marker has its particular and independent risk detection rate and the presence of several positive markers, including advanced maternal age, considerably increase the final risk of having a baby affected by T21 or some other form of chromosomal problem: Trisomies 18 and 13, Turner syndrome and Triploidies
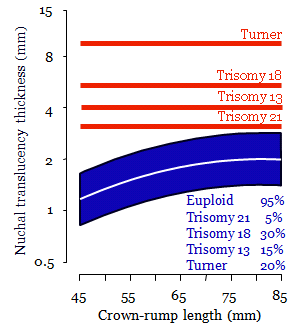
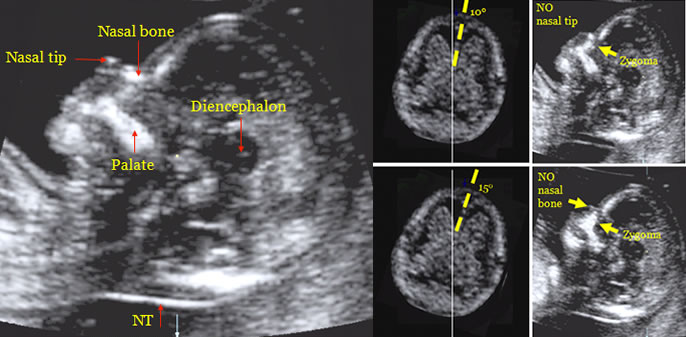
Nuchal Translucency, NT (FMF Protocol): Space between the cervical spine and the skin of the baby’s neck. It is the most important marker and the one that most frequently suggest problems; however, in most isolated cases it resolves spontaneously and the baby is healthy at birth (eg, with NT from 3.5 to 4.4 mm, 70% of the fetuses will be healthy). In general it should be less than 2.5 mm (or less than p95 for each gestational age), if this dimension is exceeded, it is considered positive and other studies will be suggested. Approximate detection for Down Syndrome: 75-80% (20-25% of Down fetuses will have normal NTs). The average NT for healthy fetuses is 2.0 mm, Trisomies 21, 13, 18 and Turner syndrome are 3.4 mm, 4.0 mm, 5.5 mm and 9.2 mm, respectively. Abnormal NT may disappear as the baby grows so that it is important to make the measurement at the appropriate time: a recent case presented TN of 4.5 mm and general edema of the fetus at week 12. In the control at week 16 all markers were within normal limits, amniocentesis was still performed and the expected abnormal Karyotype was obtained: Turner syndrome. If the study had not been performed at week 12, the diagnosis would have been delayed or missed, it would have been made very late or it would not have been done until infancy.
{kind=link}

Normal NT
Nasal Bones, NB (FMF Protocol): Babies with Down Syndrome have smaller (hypoplastic or absent) nasal bones than healthy babies. They are considered abnormal when they measure less than 2.5 mm or when they are absent. Approximate detection: 73%.
Absent in 60%, 50% and 40% of the cases of Trisomies 21, 18 and 13, respectively. It is the hardest measurement to obtain, the scanning plane must be very precise (quality control) and the baby must be still. It may be absent in 2% of healthy babies, 60% in T21, 50% in T18 and 40% in T13.
{kind=link}
Normal nasal bone
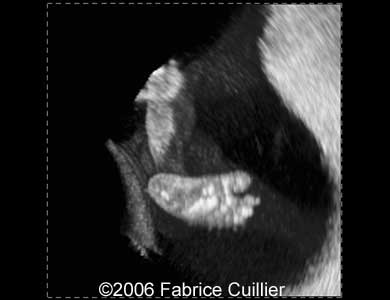
Ductus Venosus, DV (FMF Protocol): Small portion of the umbilical vein before it reaches the heart. The alteration in the shape of the flow waves obtained (reverse A wave) is considered abnormal and is present in Down Syndrome 65%, T18 55% and T13 55% and / or Congenital Heart Disease. Reported detection: 80-90% (Down), variable detection in Cardiopathies. An abnormal result can be obtained in up to 4% of healthy babies, in 80% of cases of anomalous ductal wave (Wave A reverse isolated) the pregnancy normally takes place. The study should be repeated in a few weeks when the size of the ductus has increased to rule out contamination with other nearby elements. Fetal heart ( echocardiography ) should be checked between weeks 18-23, monitor fetal growth and detect risk of preeclampsia in the uterine.

Normal ductus venosus
Tricuspid valve, TV (FMF protocol) : The evaluation of the right heart valve has value in the screening of Down syndrome and some forms of heart disease. Regurgitation during the first phase of systole with velocity greater than 60 cm/s is considered abnormal. It can be associated to fetuses with T21 (55%), T18 (30%) and T13 (30%). The joint use with DV is an excellent scheme for early detection of congenital heart disease (CHD) and the risk of fetal death. With high-resolution equipment, early Echocardiography can be practiced.
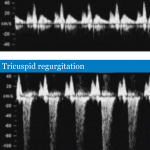
Tricuspid valve, normal and abnormal (FMF)
II General markers and other elements: they are small anatomical alterations described in different organs and systems that have been detected in a great variety of fetal anomalies. Their individual detection capacity is limited so we do an inventory of at least 10 of them, the most important and most valuable in the detection of chromosomal problems or congenital anomalies, a single positive marker may not imply the presence of problems but if we find a lot of them the risk increases considerably. In our Service we make a systematic inventory that includes the evaluation of the fetal head and its content, orbits, eyes, crystalline, integrity of the spine, thorax, diaphragm and abdominal wall; visualization of the stomach, gallbladder, bladder and kidneys; number of limbs, presence of long bones, mode of articulation, morphology of feet, hands and digital phalanges; characteristics of fetal adnexa and umbilical cord vessels. The intracardiac nucleus or nodule, the mild renal dilation and the choroid plexus cysts have little value in the absence of other markers of greater weight as described, if they are accompanied by other markers, we take them into account.
Fronto-Maxilla Angle (FMF Protocol) : The alterations of this simple measurement increase the detection of Down Syndrome but it equates to the use of a calculation program. We have not yet implemented it, we are in the evaluation phase and correct technique; I particularly report it in the presence of other altered markers since by itself it seems very subjective to me. The angle was greater than 85 ° in 69% of the T21 fetuses and in 5% of the normal fetuses. The angle decreases as the fetus grows: CRL-45mm angle: 85 °, CRL-84 angle: 77 °. This marker is very common in T18 and a little less in T21 and T13.
Heart rate: normal at 170 beats / minute at 5 weeks, decreases at 150 at 14 • In Trisomy 21 only 15% have a slight increase • In Trisomy 18 only 15% have a slight decrease • In Trisomy 13 the increase in the frequency is considerable (greater than the 95th percentile) in 85% of the cases. The inclusion of this marker is of little importance in the detection of trisomies 21 and 18 but very helpful in the 13. It does not have much value
Middle phalanx of the fifth finger: the absence of this phalanx is a relatively efficient marker to detect Trisomy 21 (36-60%) but it takes more value if it is associated with other markers

Middle 5th finger phalanx
Sole of the foot : in the fetus with T21 the first finger tends to be separated from the toe area giving the impression of having an invisible sandal, this is the sign of the Sandal or Sandal Gap
Sandal Gap (F Cuillier)
Other: lingual protrusion, double gastric chamber, renal dilation, ventriculomegaly, shortening of long bones, cardiac malformation, etc.
III Early detection of Preeclampsia risk : with new advances and a better structured study we can detect those patients who would be at risk of suffering from preeclampsia during their pregnancy, the intervention is based on the early administration of Aspirin (81 mg) from week 11 -13. There is a new calculator for early preeclampsia risk that I am implementing without considering the maternal serum markers since we do not have them and the formula works without them even though it could impair their detection capacity.
Uterine Artery: Traditionally evaluated to detect Preeclampsia risk during the third trimester (weeks 24-28) we are incorporating this element in the evaluation of the first trimester. It has a prediction rate for early severe preeclampsia with termination of pregnancy before week 34 of 80%. (FMF Protocol) .
The future is here
A diagnostic method of fetal chromosomal health is already available, which is based on the collection of fetal free DNA (cffDNA) in the mother’s circulation. The study on 864 patients had 98% sensitivity for the diagnosis of Down’s syndrome . The procedure has the approval of the FDA and the ACOG of USA but its current costs are high, hundreds to thousands of US dollars per test. Requires confirmatory studies (Amniocentesis) if there is an unfavorable result in any of the diseases
General classification of the Markers
The Combined Test is based on the combined use of the laboratory and ultrasonography in order to improve the detection rate of the most frequent chromosomal problems: Trisomies 21, 18 and 13 and Turner Syndrome. The best time to perform the Combined Test is week 11 because there is less overlap of the results of sick babies with healthy ones. With this scheme the rate of detection of fetal problems is improved and risk values ??are established that guide the obstetrician in terms of the realization, or not, of diagnostic tests such as Amniocentesis
{kind=link}
Ultrasonography : To increase the detection capacity in our Unit we established a study called Genetic Echo that includes the screening of most of the known value markers, with the intention of offering a study that discards a large number of congenital anomalies, syndromes Genetic factors and risk factors for chromosomal disorders. According to some authors, up to 90% of frequent chromosomal disorders and varying degrees (up to 100%) of many other pathological conditions could be detected.
Serological studies: Two substances of placental origin are measured in the maternal serum, the free fraction of the beta subunit of human chorionic gonadotropin (fB- hCG) and the plasma protein A associated with pregnancy (PAPP-A). Using a calculation program, the results of the Genetic Echo and laboratory tests are analyzed to generate a risk calculation for Chromosomal Disease with a detection rate of around 95%; It is the best non-genetic test that exists so far. If the test suggests high risk, the possibility of indicating and performing an Amniocentesis or similar test would be considered.
It includes:
- Nuchal translucency
- Nasal bones
- Venous Ductus
- Plasma Protein Associated with Pregnancy (PAPP-A in English)
- Free fraction of Human Chorionic Gonadotropin Sub-Unit Beta (f B -hCG)

TN and associations
The risk of Chromosomal Defects (Green), Fetal Death (Black) and Major Congenital Malformation (Red) increases in proportion to the thickness of the nuchal translucency.

In the group of fetuses with chromosomal abnormalities 50% will have Trisomy 21, 25% Trisomies 18 or 13, 15% Turner syndrome, 5% Triploidy and the remaining 10% other forms.
A higher TN greater in-uterus mortality
The higher the risk of developing severe malformations, including congenital heart disease
Mortality from syndromes, considering the 40-week pregnancy:
In utero mortality of Trisomy 21 (Down, 1/250 births) is 30%, 18 (Edward, 1/4000 births) and 13 (Patau, 1/10000 births) is 80%
The in utero mortality of monosomy X, Turner’s syndrome (Turner, 1/4000 births) is 80%.
Huggon et al. Ultrasound Obstet Gynecol 2002; 18: 610-614
TN and heart disease
Translucency also serves to detect congenital heart disease:
TN 2.5-2.9 mm 2.4%
TN 3.0-3.4 mm 2.6%
TN 3.5-4.4 mm 3.1%
TN 4.5-6.4 mm 8.3%
TN 6.5-8.4 mm 19%
TN> 8.5 mm 64.3%