- Citas Centro Médico de Caracas: Lunes, Miercoles y Viernes. Pulse el botón Agende una Cita
- Sistema de citas en linea exclusivo para Centro Medico de Caracas en San Bernardino
- Citas CMDLT: Jueves. llamar al 0212-9496243 y 9496245
- Las Emergencias son atendidas en CMDLT previa coordinacion personal al 04142708338
- Proveedor Seguros Mercantil y Sudeban

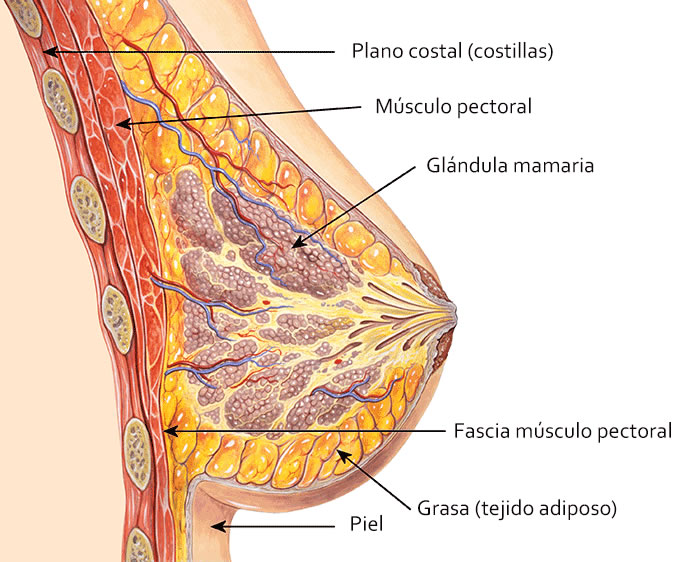
The breasts are organs that develop in the so-called “Milk Line” of mammals, which goes from the armpits to the groin, but typically located in the anterior thorax in front of the pectoral muscles, in number of two.
Mammary glands are present in both men and women, but in the latter the scarce tissue present is atrophic and nonfunctional. In women they behave as organs deeply sensitive to female hormones and especially to the hormonal changes of puberty (when they develop) and pregnancy (when they specialize).
The breasts are composed of 15-20 glandular lobes, separated from each other by fat, which drain their secretion product (milk) in the same number of lactiferous sinuses or ducts that open to the outside in 15-20 holes located in the nipples. Surrounding the nipple is a pigmented circle called areola, in its surface are about 20-25 small papules called Morgagni tubercles. The latter are the exit of sebaceous glands named Montgomery Glands that are responsible for lubricating the nipple-areolar complex, especially necessary during lactation. There is a extensive network of lymphatic vessels bellow the areolas called Sappey Plexus.
Changes during pregnancy
During pregnancy, the breasts have been strongly stimulated so that they acquire the structural and functional conditions that will allow them to adequately nourish a newborn. These changes are as follows: increased vascularity and discrete breast engorgement, glandular lobe growth and increased mammary fat content, growth and dilatation of the lactiferous channel and duct system, growth and pigmentation of the nipple, areola and the tubers of Morgagni.
Changes after childbirth
During the first 24-48 hours after a delivery or cesarean section, the reflex of descent or “lowering of the milk” occurs. Due to the effect of various hormones (oxytocin and prolactin) and the first attempts at suctioning the baby, all the glandular machinery responsible for producing milk and breast is actively stimulated in a short time, they are increased in volume, congestive, hard, hypersensitive, hot and painful. Very annoying It can even be accompanied by fever with temperatures of 38-38.5 * C. This picture is normal and due to the appearance of the breasts some authors have called it Congestive Mastitis although there is no real inflammatory process. This stage passes quickly and is improved once the mother begins to breastfeed her baby or uses the milk pump to decrease the intramammary pressure regularly.
Puerperal mastitis
Mastitis refers to a mammary inflammatory process caused by a bacterial infection. Although it can occur in women who are not breastfeeding, it is more frequent to observe this condition during the breastfeeding period when the anatomical and physiological changes suffered by the breasts, together with the local trauma exerted by the suction of the baby, make them more susceptible to suffering injuries and therefore, infections. Puerperal mastitis is exclusive of the postpartum period
This entity represents the most frequent infectious pathology of the postpartum period and probably the most frequent cause of mammary infections in the life of a woman. Despite this, the frequency with which it manifests is quite low: 1-3 cases per 100 women. Mammary infection is so rare outside of lactation that when we mention the word mastitis we automatically think about the postpartum period and breastfeeding. The infection is usually unilateral. It is striking that in spite of the repetitive trauma caused by vigorous suctioning of the baby (even when the baby already has teeth) the cases are quite few. Many of us know and many have experienced the discomfort generated by breastfeeding in its early days: pain and tear of the nipple and areola, and despite this the mother is able to continue breastfeeding without presenting major problems.
Etiology
This is a bacterial infection of the suckling breast caused by the invasion of skin bacteria through small fissures and excoriations of the areola and nipple that have been produced by the traumatic effect of sucking the baby. Typically, most cases occur in the first weeks after delivery. Although some authors say that it can occur at any time, the truth is that most of the cases that I have handled have occurred between the second and the sixth week after delivery or cesarean section. Fortunately the handling is very simple and only a couple of times I had to do some minor surgery procedure.
Symptoms
Once the bacteria have penetrated the breast tissue through excoriations of the areola or nipple, as would happen with any skin wound, the bacteria grow locally and an inflammatory reaction is generated that begins to be noticed for a bit. of pain in some of the sides of the breast, especially in the external quadrants; Afterwards, this area begins to feel warmer and a pink coloration of the skin located on the site of the infection in a triangular form begins to appear. With some frequency the patient tells that she has had some episodes of chills and fever (38-39.5 * C). She also reports that there is pain more intense to the touch or when breastfeeding the baby but when she empties the breast milk she feels a little relieved. It is possible to squeeze a certain amount of pus through some of the nipple holes. Almost invariably only one breast is affected.
Diagnosis
The diagnosis is very easy and although it could be done just by talking on the phone with the patient (this is very common in our country), this practice should be avoided since the breasts should be examined exhaustively to determine the degree of affection and rule out complications, give instructions suitable and correctly select the treatment.
Treatment options
Your doctor will indicate antibiotics, analgesics and give you specific instructions for your case. The most effective measure in handling this problem is to completely empty the breasts regularly: breastfeeding, manually or using milk pumps. Also, it is recommended to drink plenty of fluids during the day and use medications to control pain and fever if there is one. Breastfeeding is maintained using antibiotics, it is safe for the baby
What are the complications?
The most frequent complication is the Breast Abscess: when the infection is treated late bacterial growth and tissue damage are considerable, a cavity is established that is filled with pus, the breast is very inflamed, hot and with a very red zone and painful The appearance of the patient suggests illness, general malaise and fever, due to the local pain the patient does not breastfeed with the affected breast so that the milk congestion worsens even more the pain that the patient already has. This complication can appear in 5-11% of women who have mastitis.
Can I still breastfeed my baby?
Definitely you should not stop breastfeeding because, besides affecting the nutrition of your baby, milk accumulates in your breasts generating more pain and more risk of generating a breast abscess. Even when you are taking antibiotics (adequate) you should not stop breastfeeding. If you have a breast abscess, it is very likely that your doctor will try to drain it surgically or by using a puncture guided by Echo and forbid you from breastfeeding your baby. However, it will indicate that you continue to pump milk to avoid further breast engorgement.
How can I prevent it from happening to me?
The measures are very simple but the most effective is to continue breastfeeding your baby regularly.
- Frequent toilet of the nipple and areola with water. Do not use soaps or alcohol because you dry your skin by sweeping the natural lubricating fat that it produces.
- Breastfeed frequently your baby, avoid bottle feeding since you interrupt the emptying of the accumulated milk.
- Do not use overly tight bras.
- If you go to work, pump milk with milk to avoid breast engorgement.
- At the end of each period of breastfeeding you can place Vitamin E in each nipple to help keep it hydrated: you take a drop of vitamin E and place it on your finger and then apply it on both nipples. Do not use much because you may know the baby badly.
- Drink plenty of fluids during the day, water is ideal and does not get fat.
- If you have any unusual symptoms, or you feel very bad, you should immediately contact your doctor. It is never really good to self-medicate without a specialized evaluation.
Finally, remember: breastfeeding is a miracle of nature, it is inimitable and irreplaceable. Rarely is there a problem that contraindicates its use and thus, the proper attention of the breasts will prevent situations from arising that could lead to the suspension of this miraculous resource of the human species.
Anatomy
Mastitis: measures to take
- Continue breastfeeding, starting with the affected side.
- If your baby does not feel good, or does not want to suckle from the affected breast, or your discomfort is so severe that you can not breastfeed on the affected side, empty the affected breast with the breast.
- Consider lying in bed for about 48 hours.
- Take a lot of liquid.
- Decrease your salt intake
- Use the indicated analgesics/antipyretics to control discomfort and fever.
- Use cold compresses to initially control inflammation; then, use warm compresses to stimulate the descent of the milk.
- Massage the breasts from the base to the nipple to help the drainage (purulent, sometimes) in the infected breast.
- Avoid using tight bras or rigid liners.
- Wash your hands before and after handling the infected breast. You can continue to use the creams and emollients (the approved ones) of the areola and nipple.
- Avoid breastfeeding positions in which the baby has to pull your nipple a lot.
- The dose that reaches the baby is so low that you can and should continue breastfeeding.
- Contact your doctor within 48 hours of starting the antibiotic to evaluate your response: by then you should no longer have a fever and the pain will have improved markedly, as well as the red area of the breast.
- If you have not obtained improvement after the first 48 hours, plan a visit with your specialist.
Severe puerperal mastitis
This case begins as a common mastitis, note the triangular shape of the red area on the right.

The situation does not improve with the usual treatment and one begins to see an area of necrosis of the nipple and the other breast is affected. Bilateral mastitis

Necrosis progresses and treatment is changed.

Finally it improves. There was a mixture of resistant bacteria (staphylococci) and fungi (candida). This case required suspension of breastfeeding.
