- Citas Centro Médico de Caracas: Lunes, Miercoles y Viernes. Pulse el botón Agende una Cita
- Sistema de citas en linea exclusivo para Centro Medico de Caracas en San Bernardino
- Citas CMDLT: Jueves. llamar al 0212-9496243 y 9496245
- Las Emergencias son atendidas en CMDLT previa coordinacion personal al 04142708338
- Proveedor Seguros Mercantil y Sudeban

The last 20 weeks of pregnancy take place with the growth and maturation of the fetal organs until reaching the final dimensions of the moment of birth and certain basic functions that will allow it to survive in the extrauterine environment. In this period you begin to see fetal behaviors and the sense organs become active, the bones calcify considerably, the muscle mass increases, the skin thickens, the brain grows, begins to feel, hear, see and perhaps even taste . The sense of smell, who knows …
Survival begins at week 23 in Neonatal Intensive Care Units (NICU) with all available resources and advances from the developed world. The data comes from The March of Dimes and Quint Boenker Preemie Survival Foundation
Week 21: The intestinal system has developed enough to begin to digest certain substances dissolved in the amniotic fluid, even though the placenta provides almost all the food to the baby (the circulatory exchange with the mother provides glucose, fatty acids and amino acids, minerals and oxygen), this will begin to absorb the small amounts of sugar, proteins and fats (basically of cellular origin) from the swallowed amniotic fluid. During this week, the baby’s bone marrow begins to make red blood cells and other blood cells – work done by the liver and spleen to this point. Weight 360 gr and size 26 cm
Week 22: The taste buds develop, meaning that the fetus begins to distinguish flavors, which in the amniotic fluid will be very few. By this time the nerve terminals of the spinal cord reach the hypothalamus and cerebral cortex, so the baby is already able to have tactile experiences and feel pain. Up to this moment the responses to the stimulation were reflexes but from now on they are taken to the brain and located as sensation and / or pain from the point where they originate (tactile topography). Your baby can experiment by feeling his face or any part within his reach. In males, the testes begin to descend from the abdomen to the scrotal sacs, a trip that begins near the kidneys and ends in the scrotal sac. In females, the uterus and ovaries are in place – complete with a supply of follicles in their ovaries. Weight 430 gr , size 28 cm
Week 23: The lungs prepare for life outside the womb due to the development of the pulmonary alveoli (portion of the lung that is capable of exchanging gases with the blood), likewise begins the appearance of cells that produce a substance called surfactant , the substance that allows the alveoli to remain open and full of air once the baby is born and breathes for the first time. The lack of surfactant is the cause of premature babies can not breathe and manifest that picture known as Hyaline Membrane . From 12 weeks the baby shows “practice” breathing movements to help lung development; In fact, what happens is that he inhales and exhales small amounts of liquid without breathing (gas exchange) whatsoever. From the end of this week can be used drugs that accelerate lung maturation in complicated cases and at risk of premature birth, the survival of a baby in intensive care and begins to be a reality even when mortality is extremely high ( 17% of survival in very well prepared units). It weighs 501 gr and measures about 29 cm . 30% of the fetuses manifest response to light (concentrated on the maternal abdomen, flashlight, Maeda, JHMI, 2014 ). From this moment, towards the end of the pregnancy, more than 70% of the fetuses respond, but this is not true. recommends
Week 24: The sense of balance develops, the baby weighs about 600 gr and measures 30 cm . Fingerprints are formed. Thanks to a fully developed inner ear, which controls balance, your baby can have a sense of direction and know if it is upside down or face up inside the womb. The baby begins to manifest cyclical periods of sleep and wakefulness. Babies born this week have a 39% chance of survival in NICU. The odds are improved with each passing week. Despite all the advances, the complications are frequent and serious; the chances of neurological sequelae in survivors are quite high, if not unavoidable. Pulmonary maturation begins to have positive effects from this week (the pulmonary alveoli have already formed)
Week 25: The baby’s hands are almost fully developed but the nerve terminals have not completed the innervation of all their elements. Exploring the structures inside the uterus is the baby’s main entertainment. The skin has thickened a lot and it does not have that transparent aspect that allowed to see the superficial arteries and veins, it looks red and delicate but it is thick enough to be an adequate barrier; body fat is scarce but evident. It weighs 660 g r and measures 34 cm. From this moment you will gain approximately 1cm of height and 100-150gr of weight per week during the next 5-6 weeks. Survival: 50%
Week 26: The eyelids are kept closed even though the eyes are fully developed, there are eye movements but it will be about two weeks before the baby starts to open the eyes. Your baby weighs 760 gr and measures 36 cm . The eyebrows and eyelashes are very evident and the hair on the baby’s head is longer and more abundant. At this moment we begin to practice the 3D ecosonogram. Survival is around 80% . Doppler study of the maternal circulation is already adequate to predict the risk of preeclampsia in susceptible patients
The second trimester ends, the stage of fetal survival begins with rates higher than 50% in intensive therapy with somewhat more limited resources
Week 27: The baby’s lungs, liver and immune system continue to mature – and the baby has grown extremely fast: in 27 weeks, the baby’s length will have tripled or even quadrupled with respect to his measurements of the week 12. If your baby is born this week, the chance of survival is around 90% ; however, serious complications are still possible. Weight: 875 gr and size: 37 cm
Week 28: The eyes of the baby begin to open and close regularly but even if the color is already genetically determined this can only be known after 6-8 months of birth. Your baby alternates sleep / wake cycles every 20 to 30 minutes. Fetal movements become very obvious when you relax, sit or lie down, especially during the night. The facial features are very clear and the deposition of subcutaneous fat gives the baby its rounded image typical of well-nourished babies. Weight: 1005 gr . Size: 38 cm Survival: 90-95%
Week 29: The fetal movements are getting stronger, the muscle mass has increased considerably and the bones have fully developed but remain elastic, flexible and moldable (and will remain that way for a good part of their childhood). This week your baby begins to store iron, calcium and phosphorus. The movements can be so strong as to generate pain in the mother, awaken her during sleep and occasionally take her breath away. The uterus approaches the mother’s diaphragm and it becomes so heavy and voluminous that it generates discomfort, clumsiness and fatigue in the mother. Digestion is hindered by this same reason. Weight: 1153 gr . Size: 39 cm Survival: 90-95%
Week 30: The baby weighs approximately 1319 gr and measures 40 cm . The rapid weight gain phase begins with weekly increments ranging from 200 to 250 gr. The stature continues to increase at the usual rate of 1 cm per week. By this time it is very easy to detect the presence of hiccups in the baby: frequent and regular short shakes in episodes of 1-2 minutes several times a day. Hiccups are a sign of fetal well-being and have nothing to do with maternal diet. Survival: 90-95%
Week 31: In the male, the testicles continue their journey from their location near the kidneys through the groin to the scrotum, many babies are already in their final location (two white balls in the scrotum). If your baby is a female, the clitoris is almost completely covered by the smaller and larger lips, which are already clearly distinguished from each other. The lung development continues to advance but are not yet fully mature, there are still 6 weeks until the lung maturity is acquired in most babies. If your baby is born this week, the mortality will be around 5-10% and complications from prematurity (hyaline membrane, intracerebral hemorrhage, necrotising enterocolitis) will have decreased considerably; Even so, most babies will require respiratory support for a few weeks. For example, in one of my cases of prematurity managed from week 30 to week 31.5 (preterm rupture of membranes, 1600gr) the baby required ventilation for a few days and graduated from intensive therapy in 10 days without complications or sequelae. Weight: 1500 gr Size: 41 cm. Survival: 90-95%
Week 32: As of this week, it is common for patients at risk of developing preeclampsia to begin to show some changes in blood pressure or protein loss in the urine as a prelude to the onset of the disease. Your baby measures approximately 42 cm and weighs 1702 gr . Almost all babies born in this age survive the challenges of a premature birth, staying a variable time in intensive neonatal therapy and requiring assisted breathing for times also variable but increasingly smaller; some cases do not require assisted ventilation. The soft, hairy fur coat that has covered the baby’s skin during the previous months – the lanugo – begins to fall this week and, in conjunction with body fat secretions, gives the amniotic fluid a lumpy appearance; the amniotic fluid begins to look like a ripe liquid: lumpy and with ever-smaller amounts of bilirubin. The upper limit of the uterus is at a midpoint between the navel and the lower ribs. In a case of chronic fetal distress and intrauterine growth retardation, which I had recently and which required interruption of pregnancy due to imminent signs of fetal death, the baby weighed a little more than 1200 g., Was in intensive therapy only 10 days and never required support artificial respiration The child is already 15 years old and does not present any type of sequels. Survival: 95%
Week 33: The baby’s pupils begin to react to light presenting dilation or contraction according to the available levels of light inside the uterus (for example, flashlight stimulation, something that should be annoying for the baby, and which we do not recommend not at all, because we believe it is a kind of fetal torture and there is a possibility that we are altering the functioning of the fetal brain ). The weight and size continue to increase rapidly and for this week we have figures of 1918 gr and 44 cm . The lung maturity is already very close and the attention needs in therapy diminish considerably; in some cases they do not even require attention of this type, especially if they have received inducers of pulmonary maturation and are females, females breathe better than males. Survival: 95%
Week 34: The protective layer, the cheesy vernix, becomes thicker at the same time that the lanugo has almost completely disappeared, much of this has been swallowed by the baby and has become part of the meconium (fetal feces). At this time, the risk of suffering respiratory distress is less than 14% and the rest of the complications associated with prematurity are less than 1%, including neonatal mortality. Traditionally, this is the last week in which the use of inducers of lung maturation is allowed because it is considered that respiratory distress affects only a minority of premature infants (14%). Only 3 weeks left to graduate as a mature baby. Weight: 2146 gr and Size: 45 cm. Survival: 99%
Week 35 : Continues to grow and store subcutaneous fat and carbohydrates in the liver in preparation for the final stretch before delivery. The maternal womb has grown a lot and reaches almost to the lower ribs, breathing is increasingly difficult and the heaviness, clumsiness and impatience have grown considerably. The movements of the baby – baby that has almost completed its development in all the organs necessary to be born – can be so intense as to generate discomfort and pain in the mother, and weighs 2383 gr and measures 46 cm. If there is premature labor as of this week, there is no longer any formal obstetric indication to stop it or to use inducers of pulmonary maturation: the complications of treatment may be worse than those caused by borderline prematurity. The skin has finished ripening during this week, forming a protective barrier that will allow the baby’s life in his new neonatal environment and for the rest of his life. The skin, the largest organ of the human being is ready to protect the whole body, sweat, lubricate with fat and allow the growth of hair. Survival: 99%
Week 36: The baby is one step away from graduating as “mature”, continues to grow and gain weight taking advantage of his last weeks of feeding and comfort without effort. Most of the babies have matured for this moment but we continue giving them the premature delivery of labor if they were born at this moment; this is by convention, so that we all speak the same language. The amniotic fluid is clear and without bilirubin and is full of lumps of vernix caseous. It weighs 2622 gr and measures 47 cm. Survival: 99%
Week 37: Graduation week: now it is called term fetus, mature fetus, term gestation, etc. All the organs necessary to be born are considered mature and functional, now it only remains to continue growing ( 48 cm ) and fattening ( 2859 gr ) to deal with the process of birth. From this moment, it can be born and the risks or complications associated with prematurity will be less than 1% in all cases. Only the nervous system is immature and even when its maturity continues to develop it will only become effective many years after birth …
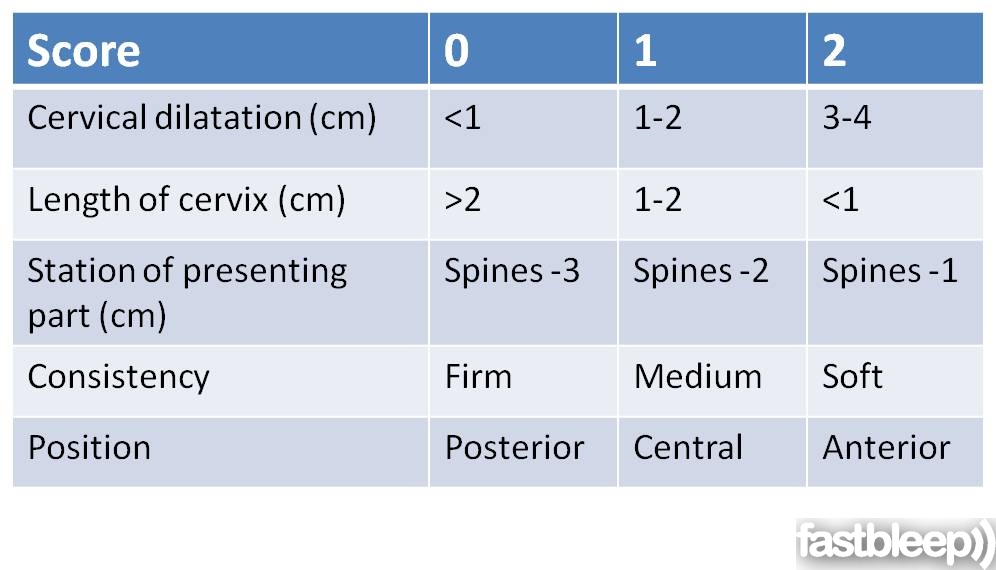
Week 38: The baby just waits, fattening and developing his nervous system, keeps growing (size: 49 cm and weight: 3083 gr ). When we plan an elective cesarean section we do it starting this week because there are recent reports suggesting that doing it during week 37 exposes the baby to a slightly higher risk of suffering respiratory distress (this does not apply to vaginal delivery). In the case of vaginal delivery, I practice an obstetric touch in order to establish the Bishop Score as an index of vaginal labor success; In addition, if I have access to the cervix I practice a Membrane Decolage (separation of the membranes attached to the cervix without breaking them) to induce the latent phase of labor and advance the level of dilation and effacement without pain until the entry by the beginning of the formal labor. Recent example, touch at 38.4 weeks with 3 cm. Start of labor 96 hours later, enter with 8 cm and little pain. Delivery completed without complications in 1 hour.
Mom very impatient , annoyed, clumsy and heavy! Everyone wants to meet the baby …
Week 39: Everything continues its normal course and the baby keeps growing (Weight: 3288 g r, Size: 50 cm ) and doing what big babies do in the womb: annoy the mother, knocking on the door, waiting to meet to his parents … The painless uterine contractions (Braxton-Hicks) have been descending to the baby, insinuating his entry into the maternal pelvis to start labor at any time. The neck has suffered shortening and possibly some degree of dilation. Mom very impatient , annoyed, clumsy and heavy!
Week 40: We arrived at the -theoretical- date of the birth. By now, most pregnant women have given birth; in fact, only 5% of women stop the day of the date of delivery calculated for their pregnancy and 97.5% of women do so between 10 days before and 5 days after this date. The placenta begins to fall short for fetal growth and the weekly growth rate begins to decline starting from this week until it becomes insufficient and an extremely dangerous condition for the baby after week 42. Mom extremely impatient, annoyed, clumsy and heavy! At any time a labor is triggered or an interruption decision is made by induction or cesarean section before week 41-42. Weight: 3462 gr and size 51 cm
End of pregnancy: if you thought that was difficult, wait and see, raising the baby is like having many births but it is also infinitely comforting. The latest that should be expected to interrupt the pregnancy is 42 weeks, the WHO recommends not to go beyond the week 41 + 3 days.
Start of pregnancy: First 20 weeks
Fetal Weight and Height: Weeks 21-40
|
Gestational age
|
Size
(cm)
|
Fetal weight
(gr.)
|
||
|
height: measured from head to toes
|
||||
|
21 weeks
|
26.7
|
360
|
||
|
22 weeks
|
27.8
|
430
|
||
|
23 weeks
|
28.9
|
501
|
||
|
24 weeks
|
30
|
600
|
||
|
25 weeks
|
34.6
|
660
|
||
|
26 weeks
|
35.6
|
760
|
||
|
27 weeks
|
36.6
|
875
|
||
|
28 weeks
|
37.6
|
1005
|
||
|
29 weeks
|
38.6
|
1153
|
||
|
30 weeks
|
39.9
|
1319
|
||
|
31 weeks
|
41.1
|
1502
|
||
|
32 weeks
|
42.4
|
1702
|
||
|
33 weeks
|
43.7
|
1918
|
||
|
34 weeks
|
45
|
2146
|
||
|
35 weeks
|
46.2
|
2383
|
||
|
36 weeks
|
47.4
|
2622
|
||
|
37 weeks
|
48.6
|
2859
|
||
|
38 weeks
|
49.8
|
3083
|
||
|
39 weeks
|
50.7
|
3288
|
||
|
40 weeks
|
51.2
|
3462
|
||
|
41 weeks
|
51.7
|
3597
|
||
|
42 weeks
|
51.5
|
3685
|
||
Macpherson T (compiler). A Model Perinatal Autopsy Protocol. AFIP. Washington DC. 1994. pages 48-54; Sung CJ and Singer DB pages 51-54.
Streeter GL. Weight, sitting height, foot length and menstrual age of the human embryo. Contributions to embryology. 1920; 11: 143-170.
Wigglesworth JS. Perinatal Pathology, Second Edition. WB Saunders Company. 1996. page 24.
I wish you the best of luck and a successful and fruitful career as parents, remember that we bring children to the world but they are not ours; our duty is to teach them to be healthy, independent, happy and successful.
*
Bishop’s score
The greater the score the better the chance to induce labor and succeed in vaginal delivery.
Scores greater than 8 are associated with figures close to 100% success
Score 6: 70% success
Scores under 6: not favorable